![]()
Executive Editor
John Reiman
The Teaching Research
Institute
Managing Editor
Peggy
Malloy
The Teaching
Research Institute
Production
Editor
Randy Klumph
The Teaching
Research Institute
In This Issue
New National Consortium on Deaf-Blindness
Activity at Home for Children and Youth Who Are Deafblind
Breaking Barriers in Asia: The Deafblind International Asian Conference
New National Consortium on Deaf-Blindness
The Teaching Research Institute (TRI) at Western Oregon University, the Helen Keller National Center (HKNC), and the Hilton/Perkins Program at Perkins School for the Blind are delighted to announce the National Consortium on Deaf-Blindness, a new national technical assistance and dissemination center for children and youth who are deaf-blind. The consortium, which began on October 1, 2006, has received funding for 5 years from the U.S. Department of Education’s Office of Special Education Programs (OSEP). It will build on the technical assistance activities of NTAC and the information dissemination activities of DB-LINK and will add a third strand related to personnel training.

The goals and objectives of the consortium are based on requirements by OSEP, outlined in a December 2005 request for applications, for a national technical assistance and dissemination center for children and youth who are deaf-blind. Staff from TRI, HKNC, and Hilton/Perkins came together in January 2006 to conceptualize and write an application. The funding award was announced this past June.
The consortium will focus on two major purposes as required by OSEP. The first is to promote academic achievement and results for children and youth (from birth to age 26) who are deaf-blind, through technical assistance, model demonstration, and information dissemination activities that are supported by evidence-based practices. Activities will be directed toward families, service providers, state deaf-blind projects, state and local education agencies, and other organizations responsible for providing early intervention, education, and transition services. The second purpose is to assist in addressing state-identified needs for highly qualified personnel who have the necessary skills and knowledge to serve children and youth who are deaf-blind. Woven throughout the proposal are activities that meet OSEP goals for accountability, highly qualified service providers, positive child outcomes, results, collaboration, and the use of effective research (to name just a few).
The consortium will continue activities historically provided by NTAC and DB-LINK, and it will also strongly emphasize new activities that promote research-to-practice and practice-to-research. I am the director, and John Reiman and Kathy McNulty are the associate directors. DB-LINK’s information services will continue, and the name DB-LINK will be used for the consortium's information service activities. The following objectives provide an overview of our activities:
- Communicate, collaborate, and form partnerships as directed by OSEP and with agencies, organizations, and projects in order to improve results for children and youth and their families.
- Implement an ongoing, multilevel needs assessment to systematically identify the needs of children and youth, their families, and service providers, including personnel training, in order to adequately and appropriately address those needs.
- Provide national leadership in the implementation of evidence-based practices to address gaps in knowledge and to scale up current practices.
- Implement an array of technical assistance and personnel-training activities to build the capacity of state and local agencies to meet the needs of children and youth who are deaf-blind and their families.
- Utilize collaborative partnerships and facilitated efforts to build the capacity of youth who are deaf-blind and their families in order to promote self-advocacy, personal empowerment, and knowledge of deaf-blindness.
- Provide leadership in a coordinated national effort to promote personnel training on the implementation of IDEA and evidence-based practices in order to address the shortage of leadership and highly qualified personnel in the field of deaf-blindness.
- Identify, collect, organize, and disseminate information related to deaf-blindness, including evidence-based practices, in order to respond to inquiries and increase knowledge that promotes effective early intervention, education, and transition services, and supports families.
- Expand the utilization of information resources by developing and disseminating accessible products that synthesize evidence-based research, effective practices, and emerging knowledge.
- Implement a comprehensive system of evaluation to assess the impact of the consortium’s objectives and activities across the four outcome domains of child, family, service provider, and systems.
We know that we cannot hope to accomplish these objectives alone. We look forward to building closer relationships and stronger partnerships among colleagues and families as we travel uncharted paths toward improving the lives of children and youth who are deaf-blind. My optimism about the collaborative work ahead calls to mind an oft-quoted phrase about success that is attributed to Henry Ford, which I paraphrase and elaborate as follows: Coming together is a beginning, working together is progress, and achieving meaningful outcomes is success.

The consortium ’s personnel, comprised
primarily of individuals who previously worked for NTAC and DB-LINK, have
extensive experience in deaf-blindness, technical assistance, and information
management and dissemination. Many staff members also work on other projects
related to deaf-blindness at TRI, HKNC, and Hilton/Perkins.
Front row, L-R: Tom Udell, Betsy McGinnity, Sarah
Beaird, Betsy Martin-Richardson, Kat Stremel, Courtney York, Barbara Purvis,
Jon Harding, Ella Taylor, Kathy McKnulty, Paddi Davies, Nancy
Steele.
Back row, L-R: Randy Klumph, Joe McNulty, John Reiman,
Gail Leslie, Steven Davies, Nancy O'Donnell, Peggy Malloy, Bernie Samples, Lisa
Jacobs, John Killoran, Mike Fagbemi, Vic Baldwin.
Activity at Home for Children and Youth Who Are Deafblind
Lauren J. Lieberman, Department of Physical Education and Sport, SUNY Brockport
Michael Pecorella, Deafblind Program, Perkins School for the Blind
Physical activity is an important part of any child’s life. Just like other children, those who are deafblind need physical activity for recreation, improving fitness, and building relationships with others. In a recent study, parents reported that their children and youth who are deafblind often have a great deal of free time but have limited recreational opportunities at home (Lieberman & MacVicar, 2003). However, with careful preparation and consideration of each child’s unique needs, healthy, productive, and rewarding physical activity experiences can take place in the home. The suggestions in this article are intended for children who range in age from pre-school to high school and who are deafblind with additional disabilities.
Before the Fun Starts: Considerations for Activities at Home
Prior to engaging in home physical activities, it is important to consider each child’s specific requirements and abilities. Parents or guardians must match physical activities and necessary supports to the unique needs of their children. For instance, when it is not safe to leave a child alone to play, a support person, sibling, or peer who knows the child well must be responsible for supervising the child and helping him or her to participate in an activity. Anyone who interacts with the child must understand his or her mode of communication, safety issues, and ability to tolerate activities. It is also important to ensure that activities are modified to meet the child’s unique needs.
To determine how best to modify an activity, consider the functional abilities of the child and the objective of the activity. For example, if a child wants to swing but has limited grip strength, tie supportive loops of Velcro and elastic or ribbon to the chains of a swing to enable the child to hold on independently. It takes time and consideration to ensure that each activity is appropriate for a child and is properly modified and safe. Adaptations to positioning, equipment, and communication strategies may be necessary. For example, Julie’s family received a side-by-side recumbent bicycle from their local Lions Club. The seat and handle bars needed to be adjusted for her size and comfort. After Julie and a friend rode the bike for a few minutes, her parents stopped the activity to check on Julie’s comfort and safety and make adjustments so she could continue to enjoy the experience.
Before beginning a home physical fitness routine, be sure to consult a physician. After that, the next steps are to set up a movement area, establish activity routines, and involve family members and friends.
Set up a movement area
It is not necessary for a movement area to take up a large amount of space. Although it is nice to have an entire room dedicated to improving personal physical fitness, that is a luxury for most people. A corner of a room or yard is sufficient. Keep the area free of hazardous obstacles that could cause injury, such as items that might be tripped over or bumped into. Keep the walls clear so that children can use them to move independently. To promote independence, give children ample time to explore and become familiar with everything in the area, including physical fitness equipment.
Establish activity routines
Set up activity routines that are familiar and have predictable outcomes. When changing a routine, discuss it with the child to make sure he or she understands the changes. It is essential to communicate in order to understand a child’s needs and desires and to set clear expectations.
Involve family members and friends
Children and youth who are deafblind often experience isolation (Kroksmark & Nordell, 2001; Petroff, 1999) and need opportunities for socialization (Haring & Romer, 1995; Smith, 2002). Experiencing physical activities with siblings, parents, neighbors, and friends can be enjoyable and memorable and promote and strengthen bonds.
It is important to educate anyone interacting with a child about his or her communication methods and any specific needs and safety precautions. For example, Jeannie loves to roll down a wedge mat in her basement. It is important for people playing with her to know that because she has certain medical needs she must do log rolls (on her side) rather than forward or backward rolls. Brian loves to play tactile twister with his family. He likes to be the spinner and make calls as well as to participate in the game. Responding to a child’s needs and wishes promotes self-determination and full enjoyment and understanding of an activity.
Preferred Activities
In a study by Lieberman and MacVicar (2003), parents identified some of their children’s favorite activities. This section reviews a number of these activities that can be enjoyed at home.
Swinging. Swings can be set up indoors or outdoors. If outdoors, ensure a clear and identifiable path to the swing-set from the house. You may want to set up a guide-wire from the house to the swing. A swing can also be set up in a garage or basement. Attach eyehooks for a swing to a wooden ceiling beam or tie the swing around a metal ceiling beam. Put mats under the swing for safety, and keep objects away from the swinging area.
Rocking. Many children enjoy rocking in a rocking chair or while sitting on a therapy ball, sofa, or chair. For example, a child can lie across a peanut-shaped therapy ball on his or her stomach with some weight on the hands while rocking forward and backward. This activity can be enjoyed inside or outside on a mat or in the grass.
Walking. Walking is a great activity both indoors and outdoors. A child can walk while trailing a wall, with friends or family members as sighted guides, or by using a guide-wire. A guide-wire is a rope or wire pulled tightly across an area such as a driveway, garage, basement, family room, or backyard. For information about how to set up a guide-wire and techniques for guided running and walking, see the Camp Abilities web site (http://www.campabilities.org). Children with sufficient vision may be able to walk independently around a yard, nearby track, or neighborhood. Walking and running can be measured using talking pedometers that can be purchased online or at any sporting goods store. A “Walk-Run for Fitness” kit will be available through the American Printing House for the Blind in the near future (http://www.aph.org).
Climbing. Climbing promotes balance, strength, spatial awareness, and self-confidence. Ladders, monkey bars, cargo nets, steps, and ramps are fun to go up, down, through, around, and inside.
Bicycling. Bicycling increases fitness and provides opportunities for socialization. Anyone who has some functional use of his or her legs can ride either a standard stationary or recumbent bike. A recumbent bike may be helpful for children with balance problems. Many stationary bikes display the distance pedaled and the amount of time ridden. Most sporting goods stores sell them for $500 to $1,000, and they can also be found in health clubs and at schools. Bicycle stands can turn an ordinary ten-speed bike into a stationary bike. “Spinning” is a popular sport offered in many health clubs, and learning how to ride a stationary bike at home can open up spinning as a future fitness activity option for a child.
Fitness Activities
It is well established that youth who are visually impaired are less physically active than their peers (Kozub & Oh, 2004) and less physically fit (Lieberman & McHugh, 2001). Any person who wants to begin improving their fitness level must build skills and increase fitness gradually. It is important to start out slowly and set realistic goals. Following are some enjoyable movement activities that promote physical fitness. Most are done using simple equipment.
Rebounders. A rebounder or mini-trampoline can be used for running in place, jumping, or bouncing. Carefully supervise the child at the beginning. Make sure there are mats surrounding the rebounder and something for the child to hold on to, such as a handrail or wall, to ensure stability and balance. This activity can also be enjoyed by jumping on an air mattress or a twin mattress, with the same precautions.
Jump ropes. Children can step over a rope held 1 to 2 feet off the ground, jump over a rope held by a peer or sibling, or jump using a handheld rope. Even children who cannot walk or stand can play by rolling over a jump rope or rolling in a wheelchair over a rope. This gives children who want to participate in the same activities as their siblings and friends a sense of accomplishment and belonging.
Children can jump rope to music, drums, or their own rhythm. They can jump a specific number of times or for a set amount of time. It is important to clearly mark a jumping area on the floor with tape or cones. A child with very limited or no vision will benefit from a change in surface around the boundary of the jumping area, like carpet squares, or from a rope taped to the floor as a tactile boundary.
Scooter boards. Children can push themselves on a scooter board while sitting, kneeling, or lying on the stomach. They can also pull themselves along a rope pulled tight close to the ground or be pulled by a family member or peer while holding on to a hula hoop, rope, or towel. As with other activities, it is essential to establish clear boundaries and use safe riding techniques and speeds. Once children have mastered movement on the scooter, they can create obstacle courses with objects to go through, under, around, and even over.
Dynabands. Dynabands are large wide stretchy bands that can be used for stretching, strengthening, balancing, and gaining spatial awareness. They come in colors that indicate different levels of tension. For Dynaband activities, consult a physical therapist or physical education teacher.
Hand weights. Hand weights can be used to increase strength. Small hand weights (3 to 10 pounds) can be purchased from any sporting goods store. In a safe corner of a room, children can do bicep curls, tricep curls, shoulder shrugs, side bends, knee bends, lunges, and side steps. These same exercises can also be done using soup cans as light weights.
Step exercises. Step exercises promote fitness, balance, and leg strength. Use a short bench (4 to 6 inches high) or commercial steps used for step aerobics. Children might set a goal to step up and down for a specified length of time, or to complete a certain number of steps, or they can just step for fun in time to music. The step should be placed in front of a wall, railing, or fence to ensure balance and safety.
Many exercises, such as sit-ups, push-ups, wheelchair push-ups, and jumping jacks, do not require equipment. All that is needed is a mat or carpeted floor and enough space for movement. See Lieberman (2005a, 2005b) for more information about adapting these fitness skills for deafblind children.
Motor Skill Activities
The fitness activities discussed above improve muscular strength and endurance, but motor skill activities help to improve agility, balance, motor coordination, manipulation skills, and eye-hand and eye-foot coordination. These skills promote independence, self-esteem, and a feeling of competence and can be very enjoyable either alone or with siblings or peers.
Ball manipulation. A ball can be rolled, kicked, or thrown against a wall or to a sibling or peer. This activity improves balance, eye-hand and eye-foot coordination, and agility. Choose a ball that the child is comfortable with. Children who have never played with a ball may need to begin with one that is not fully inflated so they are not afraid of hurting themselves. It is also important to choose a ball with a texture the child likes and that is appropriate for his or her visual capacity. For example, a dark blue or purple ball might be best for a child who sees darker colors better than lighter colors.
To help children keep track of the ball, tie it to a rope, chair, or doorknob. A ball can also be tied to a tetherball pole or volleyball post. This eliminates the need to chase or search for the ball, but care must be taken to avoid running into the central pole.
Reaching and grasping activities. Children can practice reaching and grasping using scarves, balls made of rope, beanbags, yarn balls, deflated beach balls, or a nonlatex Koosh ball. This activity helps develop hand strength, coordination, and the ability to manipulate objects with the hands. The ability to drop objects is a prerequisite for throwing, and objects can be dropped into a hula hoop, pushed off a wheelchair tray, or dropped into an eye-level basketball hoop or large garbage can.
Wedge mat activities. Wedge mats are large mats in the shape of a piece of pie on its side. The highest side may be at the level of a child’s knees or thighs. The mats can be used for log rolls, forward rolls, crawling, or tumbling. Once a child has tumbled to the end of the mat, he or she can trail it back to the top. This independent activity can be enjoyed outside on the grass or inside with the wedge mat placed on top of a flat mat. If there are safety hazards close to the play area, create boundaries using cones or rope placed within 5 to 10 feet of the mat. The wedge mat can also be set on a large mat to create a natural safety zone. Wedge mats can be purchased through equipment companies, sporting goods stores, or gymnastics programs.
Locomotor activities. Locomotor activities, like running, hopping, galloping, leaping, skipping, and jumping, work the large muscles of the legs and promote agility, coordination, gross motor skills, balance, leg strength, and endurance. For stability, they can be performed while holding onto a guide rope, wall, or fence. To learn about instructional techniques for locomotor skills, see O’Connell, Lieberman, and Petersen (2006).
Racquet and bat activities. Children can use a racquetball, badminton, or tennis racquet, or a bat, to hit balloons, small beach balls, Wiffle balls, or Nerf balls. The ball can be placed on a batting tee, thrown in the air, or dangled from a string tied to a beam or fixture. A ball can also be tied to the bat or racquet so there is no need to chase or search for the ball. Balls with bells inside are good for children who have usable hearing. Children can bat for fun, distance, and cooperative games, or bat a specific number of times.
Balance activities. A ramp, balance board, rebounder, flat curb, or balance beam can be used for balance activities. For safety, place mats under the equipment and keep the area clear. Children can challenge themselves to balance for a specific length of time or to achieve a set number of times that they walk along a beam or jump on a rebounder.
Goal Setting
It is important to remember that each child is different. Some will participate in activities because they enjoy the way a movement feels or the companionship of other participants. Others may want to become more skillful in an activity, and goal setting is an integral part of fitness, recreation, and sport. If a child’s goal is to improve, it is important to establish a baseline for activities, such as the number of push-ups, duration of walking, or accuracy or distance of ball throwing. Teaching a child how to measure improvement is a key to continued enjoyment, challenge, and success recognition. For more information on skill development and goal setting, see Lieberman, Modell, Jackson, and Ponchillia (2006).
Summary
Encouraging children who are deafblind to participate in activities at home is not always easy. It requires communication with the child, creativity, and practice, but the time and energy spent developing a variety of physical and recreational activities in the home will improve fitness, provide opportunities for fun and socialization, and open many doors for children who are deafblind.
References
Haring, N. G., & Romer, L. T. (1995). Welcoming students who are deaf-blind into typical classrooms. Baltimore: Paul H. Brookes Publishing Company.
Kozub, F. M., & Oh, H. (2004). An exploratory study of physical activity levels in children and adolescents with visual impairments. Clinical Kinesiology, 58 (3), 1–7.
Kroksmark, U., & Nordell, K. (2001). Adolescence: The age of opportunities and obstacles for students with low vision in Sweden. Journal of Visual Impairment and Blindness, 95 (4), 213–225.
Lieberman, L. J. (2005a). Deafness and deaf-blindness. In J. P. Winnick (Ed.), Adapted physical education and sport (4th ed., pp. 222–233). Champaign, IL: Human Kinetics.
Lieberman, L. J. (2005b). Visual impairments. In J. P. Winnick (Ed.), Adapted physical education and sport (4th ed., pp. 206–218). Champaign, IL: Human Kinetics.
Lieberman, L. J., & Cowart, J. F. (1996). Games for people with sensory impairments: Strategies for including individuals of all ages. Champagne, IL: Human Kinetics.
Lieberman, L. J., & Houston-Wilson, C. (2002). Strategies for inclusion: A handbook for physical educators. Champaign, IL: Human Kinetics.
Lieberman, L. J., & MacVicar, J. M. (2003). Play and recreation habits of youth who are deaf-blind. Journal of Visual Impairment and Blindness, 97 (12), 755–768.
Lieberman, L. J., & McHugh, E. (2001). Health-related fitness of children who are visually impaired. Journal of Visual Impairment and Blindness, 95 (5), 272–287.
Lieberman, L. J., Modell, S. J., Jackson, I., & Ponchillia, P. (2006). Going PLACES: Transition guidelines for community-based physical activities for students who have visual impairments, blindness, or deafblindness. Louisville, KY: American Printing House for the Blind.
O’Connell, M., Lieberman, L. J., & Petersen, S. (2006). The use of tactile modeling and physical guidance as instructional strategies in physical activity for children who are blind. Journal of Visual Impairment and Blindness, 100 (8), 471–477.
Petroff, J. G. (1999). A national transition follow-up study of youth identified as deafblind: “Parent perspectives” (Doctoral dissertation, Temple University, 1999). Dissertation Abstracts International, 60 (03A), 704.
Smith, T. B. (2002). Guidelines: Practical tips for working and socializing with deaf-blind people. Burtonsville, MD: Sign Media Inc.
Resources
American Printing House for the Blind PE Web site: “A parent/teacher resource promoting physical education and recreation for children with sensory impairments,” http://www.aph.org/pe
Camp Abilities Web site: http://www.campabilities.org
DB-LINK Web site: http://www.dblink.org (see “Play and Recreation” in the “Selected Topics” section)
The authors would like to thank Katrina Arndt for her contributions to this article
Breaking Barriers in Asia: The Deafblind International Asian Conference
Akhil Paul, Chairperson
Scientific Committee
The Second Deafblind International Asian Conference was held in Dhaka Bangladesh, in January 2006. It was hosted by the National Forum of Organizations Working with the Disabled (NFOWD), a federation of nongovernmental organizations that work with people with disabilities in Bangladesh.
Deafblind International (DbI) is a worldwide association promoting services for deafblind people. It brings together professionals, researchers, families, deafblind people, and administrators to raise awareness of deafblindness and campaign for the rights of deafblind people of all ages to have a good quality of life. The aim of this DbI Asian conference was to bring together academic experts, professionals, parents, governmental policy planners, and organizations involved in the development of services for deafblind children and adults in Asia. The theme “breaking barriers in Asia” was intended to inspire an exchange of thoughts and ideas about critical issues pertaining to deafblindness on the Asian continent. The discussions helped set up a framework for further strengthening of services in the Asian region. There were over 321 participants from 18 countries, including 72 people with disabilities. Mr. Ali Ahsan Mohammad Mojaheed, Honorable Minister, Ministry of Social Welfare, Government of Bangladesh, gave the inaugural address.
In the keynote address, Ms. Aloka Guha, chairperson of the National Trust of India, focused on the use of a human rights approach to develop services for deafblind people in the region. She urged representatives of national governments, organizations for development and disability, researchers, and deafblind people to take maximum advantage of the positive policy and legislative climate that emerged during the previous decade in the Asian region.
Many discussions and debates were stimulated during more than 70 presentations, which covered a range of topics from early intervention and identification to communication to program planning. Participants also actively engaged in discussions on the building of service capacity, the role of international and nongovernmental organizations in the region, and technology for deafblind people. There was a special focus on the importance of deafblind people speaking for themselves about their lives, their expectations, and their rights.
The resolution committee was chaired by Dr. Bhushan Punani, executive director of the Blind People’s Association in India. Resolutions included the following:
- Voice of the People: Strengthen the voices of deafblind people through all registered networks in the field of deafblindness.
- Prevention: Promote rubella immunization as a national movement in all countries in Asia.
- Standard definition: Develop a standard, appropriate definition of deafblindness to be accepted by national governments and adopted through legislative measures.
- Human Rights: Guarantee all rights for deafblind people, including the rights to work, education, quality of life, accessibility, communication, employment, and equal opportunities.
- Human Resource Development: Promote programs to train stakeholders in deafblindness, including special and inclusive teachers, caregivers and birth attendants, community-based rehabilitation workers, village health workers, interpreters, parent counselors, medical personnel, and rehabilitation professionals.
- International Recognition: Lobby the United Nations to create a new position of Assistant Secretary General on Disability Affairs and appoint a capable person with a disability to this post.
The conference proceedings are available on the Deafblind International Web site: http://www.deafblindinternational.org.
Akhil Paul is the director of Sense International (India). The organization’s Web site is at http://www.senseintindia.org.
Accommodations and Alternate Assessment Use in Schools and Programs That Serve Students who are Deaf-Blind
Stephanie W. Cawthon
School of Psychology,
Walden University
As part of a growing concern about accountability for student achievement, federal and state education agencies have implemented legislation that requires all students to participate in regular assessments of key content knowledge (No Child Left Behind Act of 2001; Individuals with Disabilities Act, 1997, 2004). All students, including students with disabilities, are to be included in these assessments. The primary method is standardized assessment, administered using multiple-choice, bubble-sheet formats. For students with disabilities, the standardized format can lead to invalid test scores. Standardized tests are not a true measure of a student’s learning because in addition to evaluating knowledge, they also measure a test-taking skill that may be hampered by a disability (Elliott & Braden, 2000; Phillips, 1994; Shriner & DeStefano, 2003).
A classic example of this problem is when a student with a visual impairment is asked to participate in a standardized assessment that is in print form. Allowing the student to complete the test in a Braille format would be considered a reasonable accommodation. A variety of testing accommodations can be implemented to make tests accessible for students with disabilities (McDonnell, McLaughlin, & Morison, 1997; Phillips, 1994). There are times, however, when there are no suitable accommodations to remove access barriers for a student with disabilities. In these cases, federal and state testing policies allow for alternate assessments for students with the most significant disabilities who cannot be reasonably accommodated on a standardized assessment (Wiley, Thurlow, & Klein, 2005).
There has been little in-depth analysis of accommodations and alternate assessment practices for students who are deaf or hard of hearing. To address this need, the National Survey of Accommodations and Alternate Assessments for Students Who Are Deaf or Hard of Hearing investigated the extent to which accommodations and alternate assessment techniques are being used for this population (Cawthon, 2006). The study was intended to serve as a starting point for understanding assessment methods used throughout the United States in a variety of educational settings. It also aimed to solicit the perspectives of those who work in the field to better guide future research and discussions of best practice.
In response to requests from educators who work with students who are deaf-blind, the survey was modified to allow participants to include information about whether their programs serve students who are deaf-blind as well as those who are deaf or hard of hearing. The summary below provides survey data specific to schools indicating that they served deaf-blind students in the 2003–2004 academic year. Forty-three schools or programs in 21 states described at least one student as deaf-blind. Nine were schools for the deaf, 23 were schools or district programs for students who were deaf or hard of hearing, and 2 were mainstreamed settings.
An important note about this study is that it requested information for each school or program as a whole. It did not request information about individual students or their assessment scores. It did seek an overall perspective on how schools and programs serving deaf-blind students (as well as deaf or hard-of-hearing students) use accommodations and alternate assessments for accountability purposes. In this way, this summary complements recent case study research conducted by Horvath, Kampfer-Bohach, & Kearns (2005).
Accommodations
The survey asked respondents about the range of accommodations used by students who participated in state standardized assessments. The most common accommodations for mathematics were the use of an interpreter,allowing students to sign responses, extended time for completion, and separate rooms. The most common accommodations for reading were the use of an interpreter, extended time, and separate rooms (see figure 1). Because of small sample sizes and large variation in responses, most of the differences between schools that served students with deaf-blindness and those that served only students who are deaf or hard of hearing were not statistically significant. Only “other accommodations” for mathematics demonstrated a difference in use between groups.

Figure 1. Reading Accomogations. (text description of chart)
Alternate Assessments
Programs that included deaf-blind students were more likely to have students participate in alternate assessments than those that served only students who were deaf or hard of hearing. The survey asked participants to indicate whether they had students participating in alternate assessments. A total of 21 schools or programs that served deaf-blind students (72%) indicated that they did. This is much higher than the percentage of programs, serving only students who are deaf or hard of hearing (43%).
Participants used a wide range of alternate assessment formats. The most commonly used formats were out-of-level testing, portfolios, and curriculum-based assessments. It is important to note that specific formats are often dictated by the policy and practices in place in each state or district. Decisions about alternate assessment formats may depend on many factors beyond the control of program staff. With this in mind, it is perhaps not surprising that there were no significant differences in alternate assessment format use between these two groups (see figure 2).
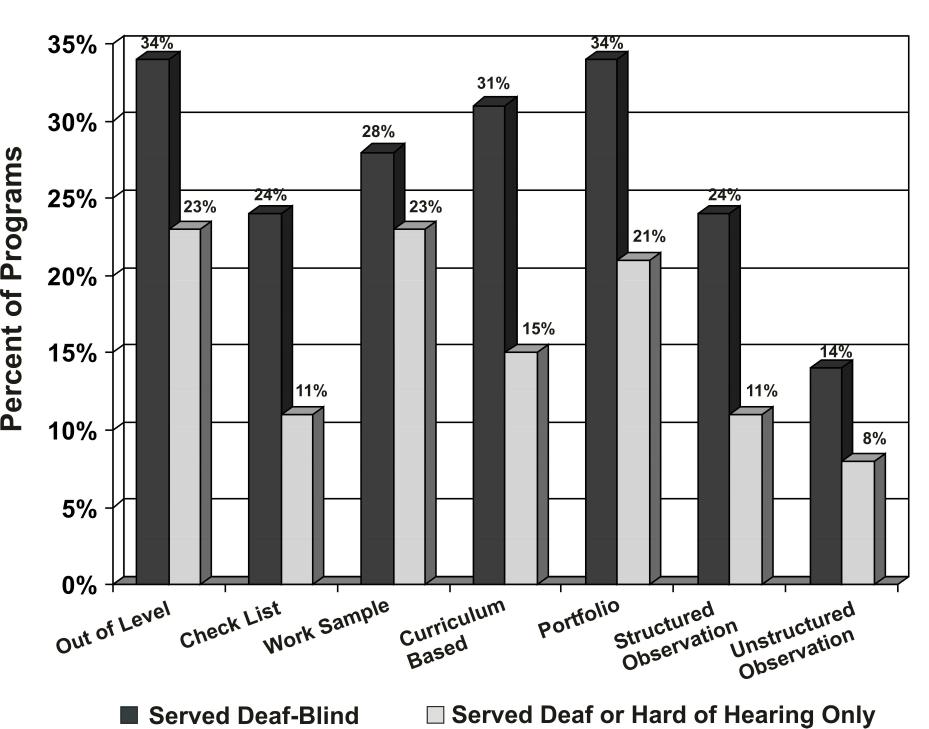
Figure 2. Alternate Assessment Formats. (text description of chart
Conclusion
Because this survey was conducted at the school or program level, the results shown here reflect only overall patterns in assessment practices with students who are deaf-blind. Future research can look more closely at these patterns by investigating practices with individual students.
Decisions regarding assessment are complex. Factors such as district and state policies, individualized education plans, instructional accommodations, available resources, and student characteristics are all important components in assessment practice. The research team hopes that this broad picture of accommodations and alternate assessment use can be a part of the larger effort of helping students who are deaf or hard of hearing, including students who are deaf-blind, to meaningfully participate in state accountability programs.
References
Cawthon, S. W. (2006). National survey of accommodations and alternate assessments for students who are deaf or hard of hearing in the United States. Journal of Deaf Studies and Deaf Education, 11 (3), 337–359.
Elliott, S. N., & Braden, J. P. (2000). Educational assessment and accountability for all students: Facilitating the meaningful participation of students with disabilities in district and statewide assessment programs. Madison: Wisconsin State Department of Public Instruction.
Horvath, L. S., Kampfer-Bohach, S., & Kearns, J. F. (2005). The use of accommodations among students with deafblindness in large-scale assessment systems. Journal of Disability Policy Studies, 16 (3), 177–187.
Individuals with Disabilities Education Act Amendments of 1997, 20 U.S.C. § 1400 et seq. (2001).
McDonnell, L. M., McLaughlin, M. J., & Morison, P. (Eds.). (1997). Educating one and all: Students with disabilities and standards-based reform. Washington, DC: National Academy Press.
No Child Left Behind Act of 2001, 20 U.S.C. 6301 et seq. (2002).
Phillips, S. E. (1994). High-stakes testing accommodations: Validity versus disabled rights. Applied measurement in education, 7 (2), 93–120.
Shriner, J. G., & DeStefano, L. (2003). Participation and accommodation in state assessment: The role of individualized education programs. Exceptional Children, 69 (2), 147–161.
Wiley, H. I., Thurlow, M. L., & Klein, J. A. (2005). Steady progress: State public reporting practices for students with disabilities after the first year of NCLB (2002–2003) (Technical Report 40). Minneapolis, MN: University of Minnesota, National Center on Educational Outcomes. [On-line]. Accessed January 3, 2006, at http://education.umn.edu/NCEO/OnlinePubs/Technical40.htm.
Research Update
Cochlear Implant Study
Ella Taylor
The Teaching Research
Institute
Western Oregon University
The Outcomes for Children Who Are Deaf-Blind after Cochlear Implantation (CIDB) Project is seeking approximately 250 children for participation in a study to determine the impact of cochlear implantation on auditory perception, language acquisition, and receptive and expressive communication. Currently, very little information is available about children who are deaf-blind and have cochlear implants. The primary goal of the study is to increase knowledge about this population. Children younger than 13 who currently use or are considering using a cochlear implant may be eligible to participate.
At the beginning of the study, four assessment questionnaires are completed for each child: three by family members and one by a state deaf-blind project staff member based on interactions with the child. Follow-up assessments depend on how long a child has had an implant. Children who have not yet received a cochlear implant or who have recently received one will have subsequent assessments every 12 months for 3 years. Children who have had an implant for less than 7 years will be assessed one more time after 12 months. Children who have had an implant for more than 7 years undergo no further assessments. A small stipend is given to families of children who qualify for participation in the study.
The CIDB Project is a joint effort by the Teaching Research Institute at Western Oregon University, the Beach Center on Disability at the University of Kansas, and the Midwest Ear Institute at St. Luke’s Hospital, in Kansas City, Missouri. Fifteen state deaf-blind projects are participating: California, Florida, Illinois, Indiana, Kansas, Kentucky, Maryland, Minnesota, Missouri, Nebraska, New Jersey, New York, Oregon, Pennsylvania, and Texas. This project (Grant #H327A050079) is funded by the U.S. Department of Education’s Office of Special Education. For more information, visit http://www.wou.edu/cidb, e-mail CIDB@wou.edu, or call 877-660-CIDB (2432).
__________________________
Adapted Prelinguistic Milieu Teaching for Children Who Are Deaf-Blind
Susan M. Bashinski
Beach Center on Disability
University of Kansas
Development of a capability for meaningful communication is a primary goal for children who are deaf-blind. Prelinguistic Milieu Teaching (PMT) strategies have been found to effectively increase the use of gestures and vocalizations by children with significantly delayed language or intellectual disability, but have not previously been adapted for children who are deaf-blind. The Promoting Communication Outcomes through Adapted Prelinguistic Milieu Teaching for Children Who Are Deaf-Blind study is being conducted to investigate the effectiveness of these strategies in improving communication outcomes for children with deaf-blindness who have not yet developed formal language skills. The study (Grant #H324D030003) is funded by the U.S. Department of Education’s Office of Special Education.
Twelve children between the ages of 3 and 8 years, from the greater Kansas City area and from Lawrence and Topeka, Kansas, are participating in the study. Two children are in the baseline phase, in which their initial status is assessed and described prior to the start of intervention. Four children are currently in the intervention phase. Six have already completed their intervention and are being monitored to see whether they maintain the communication skills gained during intervention.
During the intervention phase, which lasts several months, each child participates in one-on-one interaction sessions with a project staff member 4 out of 5 days each week. Each 45-minute session includes teaching routines designed to provide opportunities for the child to use natural gestures and/or vocalizations. The staff member follows the child’s lead to the greatest extent possible.
At the start of the study, each child communicated at a very, very low rate. That is, each child made less than one communicative attempt per minute. A communicative attempt, or act, is defined as a gesture, a vocalization, or a combination of these two, performed for the purpose of interacting with another person. Examples include a child’s raising a hand to give a “high five” to another person, taking another person’s hand and moving it to a desired toy, or extending a hand with palm up to request an item. The goal for this study is to increase the number of communicative acts by each child to at least one per minute for the duration of a 45-minute session over three consecutive videotaped sessions (one session videotaped with each child each week). So far, five children have met or exceeded this goal. The overall average communication rate, when intervention ended for each of the six children, was 1.52 communication acts per minute. This means that, on average, the children communicated, without prompting, an average of 68 times during each 45-minute session. All of the children, including one child who did not achieve the target goal because of motor challenges, showed significant increases in their rates of communication and in the diversity of ways that they communicated.
This study is now being repeated in Indiana. The Indiana Deaf-Blind Project has identified six children who will participate in the intervention and be evaluated using the same procedures as in the Kansas study.
As a result of this research, children who are deaf-blind are demonstrating progress, most of them significant progress, in learning prelinguistic communication skills. More importantly, they are learning the power of communication—an essential bridge to symbolic forms of communication. It is hoped that families of children with deaf-blindness will also benefit from this study. As a result of their children’s increased communication skills, families might experience more enjoyable interactions, reduced frustration, and increased participation by their children in family activities. The study’s positive results provide concrete support for intensive application of adapted PMT strategies, and might be used by families to advocate for this service. State deaf-blind projects may also benefit by sharing information about this evidence-based strategy with special education administrators and local school teams. For more information, contact Susan Bashinski by phone at 785-864-2459 (voice) or 785-864-3434 (TTY), or by e-mail at sbashins@ku.edu
__________________________
Publication on Research-Based Instructional Strategies for Students with Disabilities
The Access Center in Washington, DC, has developed Strategies to Improve Access to the General Education Curriculum. This is a periodically updated chart that identifies educational practices that are either backed by evidence or are promising but need more validation. Strategies include computer-assisted instruction, differentiated instruction, peer-assisted learning, professional collaboration, adapted books, literacy-rich environments, curriculum-based measurement, and functional behavioral assessment systems. The chart can be accessed at http://www.k8accesscenter.org/documents/InstructionalMethodsandPractices_3-16.pdf
__________________________
What Works Clearinghouse Help Desk
The What Works Clearinghouse’s Evidence-Based Education Help Desk provides federal, state, and local education officials, researchers, program providers, and educators with practical, easy-to-use tools for rigorous evaluation of educational interventions and identification and implementation of evidence-based interventions. The Help Desk is operated by the What Works Clearinghouse of the U.S. Education Department’s Institute of Education Sciences. Call the Help Desk toll free at 866-992-9799 for help in using and finding resources, or e-mail info@whatworkshelpdesk.ed.gov. See the Web site at http://www.whatworkshelpdesk.ed.gov.
__________________________
If you have information that you would like to include in “Research Update,” contact:
Peggy Malloy
malloyp@wou.edu
503-838-8598
(V/TTY)
Deaf-Blind Perspectives
Teaching Research Institute
345 N.
Monmouth Ave.
Monmouth, OR 97361

For Your Library
Going PLACES: Transition Guidelines for Community-based
Physical Activities for Students Who Have Visual Impairments, Blindness, or
Deafblindness
Lauren Lieberman, Scott Modell, Ileah Jackson, &
Paul Ponchillia. (2006). Louisville, KY: American Printing House for the Blind.
Going PLACES is a resource guide for teens and young adults that promotes independent physical activity. It outlines a step-by-step process for choosing and participating in sports and other physical activities outside of the school arena. It includes worksheets for choosing an activity, descriptions of activities, modifications and accommodations, suggestions for skill development, information about safety and self-advocacy, and athlete profiles that encourage a healthy lifestyle. It is available in large print and Braille formats, both of which come with a CD-ROM version (standard text). Cost: $68.00. To order, contact the American Printing House for the Blind. Phone: 800-223-1839. E-mail: info@aph.org. Web: http://www.aph.org.
Touch of Home. . . Road to Realizing a Vision
Betsy
Hodge & Monika McJannet-Werner. (2006). Liberty Corner
Enterprises, Inc. and Helen Keller National Center.
Deaf-blind people with additional and complex challenges are often underserved. This 48-page publication describes a model for the development of a program to successfully support deaf-blind individuals in a setting that offers not only a housing option, but vocational choices and opportunities to participate in the dynamics of a community. It is a program that reflects life, rather than life being run on a program. Touch of Home was developed through a collaborative process that included local entities and services in the Asheville, North Carolina area and a partnership with Liberty Corner Enterprises, an affiliate program of the Helen Keller National Center (HKNC). The monograph was written in response to many inquiries received regarding the development of the project, and to encourage others to develop similar resources in their own community. Single copies can be obtained free of charge by contacting Rob Ruis at rruis@libertycornerent.com, or Monika Werner mw4HKNC@aol.com. The document can also be downloaded from the HKNC web site, http://www.hknc.org. It is available in alternative formats.
Tactile Strategies for Children Who Have Visual Impairments and
Multiple Disabilities: Promoting Communication and Learning Skills
Deborah Chen & June E. Downing. (2006). New York: AFB Press.
This book is designed to teach service providers and family members how to interact through touch with children who need tactile information to support their learning. Topics include the sense of touch, support of interactions through touch, assessment of tactile skills and planning of interventions, consideration of multiple communication options, adaptation of manual signs to meet a child’s needs, selection and use of appropriate tactile strategies, and encouragement of emerging literacy. Cost: $39.95. Available from AFB Press. Phone: 800-AFB-LINE (232-5463). E-mail: afborder@abdintl.com. Web: http://www.afb.org.
From Russia with Love and Care for Children with Multiple
Disabilities and Challenging Behaviour: A Demonstration Model [CD-ROM]
Jan van Dijk, Catherine Nelson, & Ton van der Meer. (2006).
This interactive CD-ROM is the result of cooperation between the authors and staff members of the Children’s House at Sergiev Posad in the Russian Federation. From 2000 to 2005, the group collaborated as they studied children with multiple sensory impairments and moderate to severe challenging behaviors. The behaviors of six children are analyzed through video analysis, A-B-C analysis, and direct observation. Interventions and follow-up measures are included. For a more detailed description, see http://dblink.org/newpub.htm. Cost: $45.00. Order by sending a check to Mr. Joe Franken, 4619 Spyglass Drive, Dallas, TX 75287. Write “From Russia” on your check.
Teaching Language Arts, Math, and Science to Students with
Significant Cognitive Disabilities
Diane M.Browder & Fred Spooner
(Eds.). (2006). Baltimore: Paul H. Brookes Publishing Co.
The purpose of this book is to show meaningful ways for educators to help students with significant cognitive disabilities to meet the expectations of the No Child Left Behind Act with regard to progress in reading, math, and science. It includes chapters on promoting access to the general curriculum, building literacy at the presymbolic, early symbolic, and reading levels, enhancing numeracy, and teaching math and science functional skills in accordance with the act’s standards. Cost: $49.95. Available from Paul H. Brookes Publishing Co. Phone: 800-638-3775. E-mail: custserv@brookespublishing.com. Web: http://www.brookespublishing.com
Proceedings of the Summit on Cerebral/Cortical Visual
Impairment: Educational, Family, and Medical Perspectives, April 30,
2005
Elizabeth Dennison & Amanda Hall Lueck (Eds.). (2005). New
York: AFB Press.
This summit brought together educators, medical professionals, and families to discuss issues related to cortical visual impairment (CVI). Panels considered the following topics: the definition of CVI, clinical and functional measures used to identify children with CVI, how brain research can be integrated into education and rehabilitation of children with CVI, available evidence that can be used to serve children with CVI, and research and training needs in the field. Cost: $39.95. Available from AFB Press. Phone: 800-AFB-LINE (232-5463). E-mail: afborder@abdintl.com. Web: http://www.afb.org.
CHARGE Syndrome: A Management Manual for Parents
Meg
Hefner & Sandra Davenport (Eds.) (2002). CHARGE Syndrome Foundation.
This manual, published in 2002, is now available online as an interactive publication in Adobe PDF Format. It includes information about the medical aspects of CHARGE, development and education, and resources. The manual is also available in Spanish (must be ordered offline). Web: http://chargesyndrome.org/resources-manual.asp
Conferences and Events
8th International CHARGE Syndrome
Conference
July 27–29, 2007
Costa Mesa California
For information contact the CHARGE Syndrome Foundation, Inc., 409 Vandiver Drive, Suite 5-104, Columbia, MO 65202. Phone: 800-442-7604. E-mail: info@chargesyndrome.org. Web: http://www.chargesyndrome.org/conference-2007.asp.
__________________________
14th Deafblind International World
Conference
September 25–30, 2007
Perth, Australia
Exciting international and national speakers will form part of the conference program based around the theme, “Worldwide Connections: Breaking the Isolation.” An estimated 1000 delegates will attend from throughout the world. Participants will include international, national, and local health and disability professionals and service providers; recognized experts in deafblindness; and representatives from the international blind and deafblind communities. For more information contact Senses Foundation, Inc., P.O. Box 14, Maylands WA 6931, Australia. Phone: 61 8 9473 5400. TTY: 61 8 9473 5488. E-mail: conference@senses.asn.au. Web: http://www.dbiconference2007.asn.au.
__________________________
Helen Keller National Center National Training Team Seminars
The Helen Keller National Center National Training Team (NTT) was established to increase knowledge and support the development of skills specific to deaf-blindness in individuals working with consumers who are deaf-blind across the country. The NTT holds numerous seminars throughout the year. The 2007 schedule was not available at the time this issue of Deaf-Blind Perspectives went to press. For up-to-date information, check the NTT web page (http://hknc.org/FieldServicesNTT.htm) or contact Doris Plansker, NTT Administrative Assistant. Phone: 516-944-8900, ext. 233. TTY: 516-944-8637. E-mail: ntthknc@aol.com.
__________________________
Addressing the Needs of Students Labeled Deaf and
Low Functioning, Deaf-Blind, or At-Risk Institute
March 28–30,
2007
Houston, Texas
An overwhelming majority of students who are deaf, hard of hearing, or deaf-blind do not transition to college. There are many factors that contribute to this—during childhood, as well as during and after transition from high school. This conference will provide opportunities to learn from national and state leaders about educational, rehabilitation, home, and job training strategies. For more information contact Theresa Johnson, Education Specialist, 7145 West Tidwell, Houston, TX 77092. Phone: 713-744-6391. E-mail: tjohnson@esc4.net.
Announcement
New Deafblind International Rubella Network
Deafblind International recently approved a new Rubella Network. Although the Centers for Disease Control and Prevention announced in 2005 that rubella had been eradicated from the United States, the World Health Organization estimates that annually, 100,000 children are born with congenital rubella syndrome (CRS) worldwide. CRS can cause deafness, blindness, heart problems, and a host of other health issues in babies born to mothers who contract rubella during the first trimester of pregnancy. Of grave concern, is the onset of additional health problems as these children age. The network will establish an international platform from which information and research about rubella and CRS can be shared. For more information, contact:
Nancy O’Donnell
Helen Keller National Center
141 Middle
Neck Road
Sands Point, NY 11050
HKNCNOD@aol.com
516-944-8900, Ext. 326
Back Issues of Deaf-Blind Perspectives
Back issues of Deaf-Blind Perspectives, beginning with the first issue published in September 1993, are available online at http://www.tr.wou.edu/tr/dbp. The following is a list of some of the articles, essays, poems, and research updates that can be found on the web site.
Feature Articles
- Cochlear Implants for Young Children Who Are Deaf-Blind
- Classroom Observation Instrument for Educational Environments
- Project SALUTE Information Sheets: A Field Test of the Spanish Translation in Puerto Rico
- Understanding Balance Problems in Children with CHARGE Syndrome
- A Personal View of Changes in Deaf-Blind Population, Philosophy, and Needs
- No Teacher Left Behind: Training Teachers to Meet the Challenge of Accessing the General Curriculum for Deafblind Students
- Computer Activities to Support Communication and Language Development
- Capturing Change: Measuring the Impact of An Interagency Transition Team Approach
- PHASES: Psychologists Helping to Assess Students’ Educational Strengths
- Grade One Braille for Students Who Are Deafblind
- Resonance Boards
- Intervenor Training
Additional Articles
- Project SPARKLE
- Forty Years After the Epidemic: HKNC Hosts an International Symposium on Rubella
- Getting In Touch: The Perkins Museum
- DVD/Video Review: We Have Contact!
- Learning From Children Who Are Deafblind: “Throw Away the Toys”
- Communication Portfolio: A Tool to Increase the Competence of Communication Partners of Learners Who Are Deafblind
- Ready for Partnership: Collaboration Between NFADB and State Deaf-Blind Projects
- Deafblindness in Australia: The State of the Nation
- Oregon Deafblind Project Intervener Training Program
- Deafblind International World Conference on Deafblindness Workshop Presentations
- Mississippi’s Deaf-Blind Focus
- Assessment as a Creative Action
- AADB Mentoring Project
- Collaboration Achieves Travel Success
Essays/Poems
- Our Experiences (to Date) with Sam’s Cochlear Implant
- Fifteen Today (poem)
- Guardianship (poem)
- Personal Perspectives: Selecting the Right Assistive Technology for Me
- Personal Perspective: Being More DeafBlind
- Personal Retrospective: Roberta Reid
- Siblings: Unusual Concerns…Unusual Opportunities
- Personal Perspectives: Ron Relaford
- Spotlight on Assistive Technology
- The Silent Dark (poem)
- He Didn’t Listen (poem)
- Personal Perspectives: Stephanie MacFarland
Research Update
- The “Struggle to Symbolism” Studies
- Functional Hearing Inventory: Project to Identify Criterion-Related Validity and Interrater Reliability
- Promoting Communication Outcomes through Adapted Prelinguistic Milieu Teaching for Children Who Are Deaf-Blind
- Assessment Project Update: Validation of Evidence-based Assessment Strategies to Promote Achievement in Children Who Are Deafblind
- Persons Aging with Hearing and Vision Loss
In Every Issue
- For Your Library (New Products and Publications)
- Announcements
- Conferences & Events